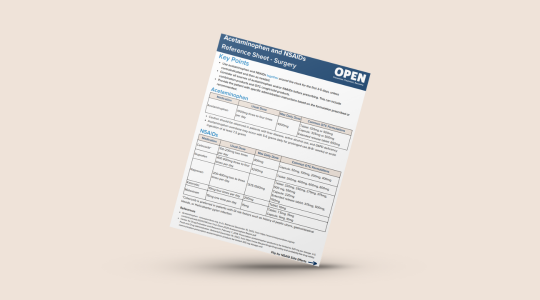
Learn more about prescribing acetaminophen and NSAIDs for pain management after surgery.
____________________________________________________________
Cite this work:
OPEN: Overdose Prevention Engagement Network (2024). Acetaminophen and NSAIDs Reference Sheet- Surgery. Retrieved from https://doi.org/10.56137/OPEN.000039