OPEN is committed to supporting evidence-based policies to improve opioid prescribing and disposal. Legislation at the state and federal level can help address the many complex issues related to opioid overuse and overdose. Policies implemented in the state of Michigan cover a variety of opioid related topics, including prescribing controlled substances, overdose treatment, medications for opioid use disorder, naloxone, and the non-opioid directive.

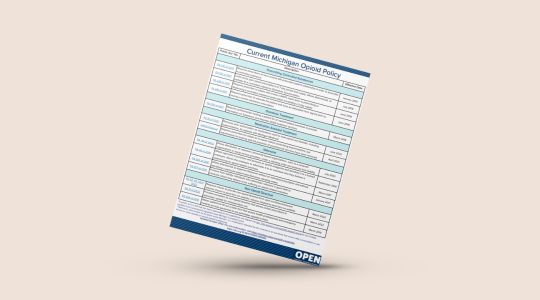
| Jurisdiction | Bill Number | Summary | Status | Last Activity |
|---|---|---|---|---|
| State | SB 0133 | Overdose Fatality Review Act: allows a county to establish an overdose fatality review team and prescribe its membership, set duties and responsibilities, submit annual report, confidentiality requirements | Ordered enrolled (passed by Senate and House) | 11/9/23 |
| State | HB 5178 | Provide for syringe service programs | Referred to committee | 10/18/23 |
| State | HB 5179 | Modify definition of drug paraphernalia | Referred to committee | 10/18/23 |
| State | HB 4734 HB 4735 HB 4736 HB 4737 | Require school districts to obtain naloxone and distribute to schools; require local govt. to provide access to naloxone; and require local govt. to provide training | Referred to committee | 6/14/23 |
Table last updated: 12/5/23
OPEN’s policy mission is to develop and disseminate evidence to policy-relevant audiences in order to increase knowledge and promote best practices surrounding acute care episodes to improve treatment, outcomes and overall health.
Opioids are commonly prescribed after surgery for pain management and many patients receive their first exposure to opioids following surgery. Prescribers have little guidance available on opioids and overprescribing is a widespread problem that contributes to the opioid epidemic currently claiming 130 American lives every day. With up to 92% of patients having leftover opioids after common operations, millions of pills are left vulnerable to diversion into communities.
Key Takeaways:
Resources:
Key Publications:
Opioid prescribing increased 68% from 2010 to 2016 in the field of dentistry. Many people are exposed to opioids for the first time after dental surgery, such as wisdom tooth removal. Patients who took opioids reported higher pain, and there was no difference found in satisfaction between patients who took opioids and who did not.
Key Takeaways:
Resources:
Key publications:
Surgical and dental procedures are among the most frequent indications for opioid prescriptions to adolescents and young adults. Rates of new persistent opioid use among pediatric patients are comparable to those for adults, with 4.8% of patients refilling opioid prescriptions between 3 and 6 months after surgery.
For more information on OPEN’s current projects: https://michigan-open.org/peds
Key publications:
Among surgical patients who developed new persistent opioid use, surgeons provided the majority of opioid prescriptions during the first three months after surgery. By nine to twelve months after surgery, however, the majority of opioid prescriptions were provided by primary care physicians. Enhanced care coordination between surgeons and primary care physicians can allow earlier identification of patients at risk for new persistent opioid use to prevent misuse and dependence.
For more information on current projects: https://michigan-open.org/initiatives/transitions-of-care/
Key publications:
While there is a growing prevalence of naloxone fills among insured U.S. adults receiving opioids, overall prevalence of naloxone prescribing remains extremely low. Key factors associated with opioid overdose risk were also associated with receiving naloxone. However, history of overdose was not associated with filling a naloxone prescription. Substantial further work is needed to increase naloxone access for patients at risk for opioid overdose.
For more information on current projects: https://michigan-open.org/medic/
Key publications:
6.0% of pregnant women filled an opioid prescription during pregnancy, and 4.0% of the women who filled developed new persistent opioid use. Having a non-delivery procedure in pregnancy and having an emergency room visit during pregnancy are factors associated with filling an opioid in pregnancy. Filling a peripartum opioid prescription (1 week prior to or 3 days post-discharge) was significantly associated with new persistent opioid use.
Key publications:
| Public Act* No. | Description | Effective Date |
|---|---|---|
| Prescribing Controlled Substances | ||
| PA 247 of 2017 | Requires prescribers to have a bona fide prescriber-patient relationship in order to prescribe a controlled substance. | Jan 2019 |
| PA 251 of 2017 | Limits acute pain opioid prescriptions to 7-day period and supply. Allows pharmacists to partially fill a controlled substance (Schedule 2) prescription. | July 2018 |
| PA 248 of 2017 | Requires prescriber to obtain and review a MAPS report prior to prescribing or dispensing a controlled substance prescription exceeding a 3-day supply. | June 2018 |
| PA 246 of 2017 | Requires prescriber to educate the patient and have an attestation form signed prior to issuing a control substance prescription. | June 2018 |
| Overdose Treatment | ||
| PA 250 of 2017 | Requires professionals treating a patient for an opioid-related overdose to provide information on Substance Use Disorder (SUD) treatment services. | March 2018 |
| Medication Assisted Treatment | ||
| PA 19 of 2022 | Removes prior authorization on medications used to treat opioid use disorder, including buprenorphine, for patients with Michigan Medicaid. | June 2022 |
| DHHS (Federal) | Requires prescribers to obtain an X-waiver before prescribing buprenorphine, but requirements for training and the provision of psychosocial services have been removed. | April 2021 |
| Naloxone | ||
| PA 176 of 2022 | Allows the distribution of naloxone community-based organizations, such as a nonprofit organizations or social service providers, under a standing order and protects from liability. | July 2022 |
| PA 39 of 2019 | Allows agencies to purchase and possess an opioid antagonist and distribute it to a trained employee. Allows the employee to administer it to an individual who they believe is experiencing an opioid-related overdose. | Sept 2019 |
| PA 383 of 2016 | Allows pharmacists to dispense Naloxone without an individual prescription and without identifying a particular patient (aka Naloxone standing order). | March 2017 |
| PA 307 of 2016 | Protects from liability individuals who administer naloxone in good faith to someone whom they believe to be suffering an opioid-related overdose. | Jan 2017 |
| Non-Opioid Directive | ||
| PA 42, PA 43, PA 44 of 2022 | Requires insurer to provide non-opioid directive form upon enrollment/renewal; requires insurer to post form on website; requires hospital to post form on website. | March 2022 |
| PA 41 of 2022 | Provides exception to non-opioid directive that allows certain prescribers to administer opioids for intraoperative use. | March 2022 |
| PA 554 of 2018 | Allows patients to fill out a state form that directs health professionals and emergency medical services personnel to not administer opioids to them. | March 2019 |
Table last updated: October 2022
*A public act is a bill that has been approved by the Legislature and signed into law. This version is as originally passed and does not include updates from subsequent legislation (see Michigan Compiled Laws).
**Naloxone, also known by its brand name Narcan®, is a medication intended for the reversal of an overdose that occurs after consumption or use of one or more opioids or opioid-related substances.
MAPS is a prescription drug monitoring system (PDMP) that helps keep track of the prescription of controlled substances through an electronic database. Controlled substances tracked (schedules 2 – 5) have an accepted medical use, such as opioids, stimulants, depressants, hallucinogens, and anabolic steroids. MAPS helps protect patients by:
For PDMPs to be most effective, states must work together to improve accessibility, ease of use, and the transparency of PDMPs across state lines. Electronic interstate data sharing will aid in increasing PDMP data’s utility, enhancing patient care, and avoiding drug diversion and misuse. This is crucial as evidence suggests that patients cross state lines in order to seek pain management options and avoid detection by PDMPs.3 In addition, integration of EHR systems, real-time data updates, improved accessibility and ease of use, and access delegation are all critical facilitators that may help improve PDMP implementation and efficacy.4
Integration may lead to greater efficiency by:
Data from MAPS offer valuable insights into opioid and other controlled substance prescribing and help improve patient health, clinical care, and research. These insights can be uniquely identified through secure connections with other health information. Analyses of the combined data sources can uncover nuanced patterns and specific opportunities to improve prevention efforts and patient outcomes in Michigan.
Using securely linked maps data, we can address these areas:

Use this two-page document to share how safe and secure access to data from Michigan’s prescription drug monitoring program can improve patient health, clinical care, and research.
Older persons usually consume less opioids after surgery, but MAPS data helped to identify that vulnerable Michigan patients with frailty have higher needs for opioids after surgery.5
MAPS data was used to pinpoint how patients are at risk of long-term opioid use after surgery because of excess prescribing, not the opioid prescription itself, highlighting the importance of reducing excessive prescriptions.6
While opioid prescribing recommendations can help surgeons reduce excess prescriptions, patients that were exposed to opioids before surgery are often excluded. Using MAPS data, researchers are able to tailor recommendations to better meet the needs of patients who use opioids before surgery.7
By studying how health outcomes for people on long-term opioid therapy for pain are impacted by insurance status, MAPS data was used to better understand the care provided for Michigan Medicaid patients.8
Establishing a policy that provides a clear and specific method for accessing MAPS data for research can help ensure the ongoing discovery of findings that improve health and wellbeing, while also keeping data safe and secure. It is recommended that policymakers consider both data access and data safety and security when developing such a policy.
For more information on the role of MAPS data in research, and what elements can help ensure safe and secure data access, such as data sharing agreements and honest broker systems, view the policy brief below:
How will the Michigan opioid laws impact your care?
Before you receive a prescription, your doctor:
*MAPS, Michigan Automated Prescription System, is a tool that tracks past and current prescriptions written for you.

This resource helps patients understand requirements and limitations, mandated by Michigan law, when writing for prescription opioids.